Sudden Unexpected Death Due to Myocarditis Caused by Coronavirus Disease 2019: Postmortem Histopathologic Evaluation
Article information

Trans Abstract
Coronavirus disease 2019 (COVID-19) is a manifestation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and its major symptoms include pulmonary complications, such as pneumonia. However, it also involves the cardiovascular system and the developed myocarditis can lead to sudden unexpected death. Herein, we present a case in which a patient died four days after release from isolation due to SARS-CoV-2 infection. SARS-CoV-2 was confirmed again during postmortem (PM) inspection at the scene of death. Autopsy revealed myocarditis and evidence of pulmonary involvement with SARS-CoV-2. Pathological examination revealed myocardial perivascular infiltration of lymphocytes and macrophages with multifocally injured cardiomyocytes. The pathological findings of COVID-19–induced myocarditis differ from those of other viral myocarditis, and we assume that different pathophysiological mechanisms could have been responsible for this manifestation. After a comprehensive PM examination, including gross dissection, microscopic examination, PM computed tomography, and PM laboratory tests, the cause and manner of death were determined to be myocarditis caused by COVID-19 and naturally, respectively. This case highlights the significance of autopsy and comprehensive PM examinations in both forensic and public healthcare systems.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) belongs to the beta subgroup of coronaviruses. It is a single-stranded RNA virus with a glycoprotein envelope and polysaccharide-coated spike proteins covering its surface [1]. Located within the S1 subunit, the receptor-binding domain is responsible for attaching angiotensin-converting enzyme 2 (ACE2) receptors to the host cell, thereby facilitating viral entry into target cells [2]. The ACE2 receptor is expressed abundantly in type II pneumocytes, as well as in cardiovascular, renal, and gastrointestinal tissues, accounting for the pathogenesis, multi-organ involvement, and clinical manifestations of coronavirus disease 2019 (COVID-19) [3].
Myocarditis refers to the inflammation of the myocardium due to various infectious and non-infectious etiologies [4], with viral infection being the most important cause [5]. The virus in the beta-coronavirus group can cause myocarditis. And immune-mediated and toxic myocarditis has been reported as well [5]. SARS-CoV-2 may invade cardiac myocytes via its surface ACE2 receptors, which may cause direct cellular damage. However, the exact pathophysiology of myocarditis caused by SARS-CoV-2 remains unclear and several theories have been proposed [4]. Consequently, cardiac manifestations including myocarditis are potentially severe and lethal complications of COVID-19.
Herein, we present a case of sudden unexpected death (SUD) due to myocarditis, a fatal complication of COVID-19, with a focus on presenting its pathological findings. The patient died four days after being released from isolation due to SARS-CoV-2 infection. This case could be helpful to forensic as well as the public healthcare system.
Case Report
The deceased patient was a 68-year-old woman who was found at home, complaining of dyspnea; and her husband called for 119-emergency services. She was transferred to the emergency room, and cardiopulmonary resuscitation (CPR) was performed. However, the patient died several hours after admission. SARS-CoV-2 was confirmed using a polymerase chain reaction test 10 days before the patient died. Subsequently, the patient was isolated for one week. During isolation, she had respiratory symptoms, such as a sore throat, although it improved with painkillers. She experienced syncope after release from isolation; however, she ignored this transient symptom. After death, SARS-CoV-2 was confirmed again from the nasal swab specimen sampled during the postmortem (PM) inspection at the scene of death (Fig. 1).

Timeline of death and postmortem examination. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
An autopsy was performed within two days after death with a court-issued warrant at the request of the public prosecutor. She had a well-nourished body contour and body mass index of 29.2. External examination revealed no injuries other than CPR marks. On internal examination, the heart was grossly unremarkable, except for cardiac hypertrophy (506 g), and severe atherosclerosis was identified in the left anterior descending coronary artery. The weights of the right and left lungs were 768 g and 654 g, respectively. Both lungs were congested and a white froth was noted in the trachea and main bronchi. Mild fatty liver was noted, and sclerotic changes were observed in both kidneys. The other internal organs demonstrated unremarkable findings. Sudden cardiac death was assumed to be the cause of death after gross dissection.
PM computed tomography (PMCT) revealed livor mortis in both the lungs. However, pneumonic infiltration was not evident on PMCT. Seven formalin-fixed paraffin-embedded blocks were prepared for microscopic examination of the pericardium and heart as follows: pericardium, anterior, lateral, posterior, inferior wall of the left ventricle, interventricular septum, and right ventricle in the same short-axis section. Microscopic examination of the pericardium and heart revealed no pericarditis or epicarditis, although lymphocytic myocarditis was noted in the left and right ventricles and the interventricular septum. Lymphocytic infiltration was prominent in the perivascular spaces (Fig. 2). Myocardial infiltration of T lymphocytes and macrophages was confirmed using immunohistochemical staining. Furthermore, injured cardiomyocytes were multifocally identified using immunohistochemistry and Masson's trichrome staining (Fig. 3). Diffuse alveolar damage, intra-alveolar and interstitial edema, and lymphocytic infiltration were focally observed in the lung tissue (Fig. 4). The PM blood glycated hemoglobin level was 10.0% (reference range, ≤6.5%). However, biochemical analysis of the vitreous humor revealed a non-lethal glucose concentration (265.7 mg/dL). PM blood ketone levels were normal (beta-hydroxybutyrate, 39 mg/L; acetone, <10 mg/L). The PM blood C-reactive protein (CRP) level was 8.50 mg/dL (reference range, ≤1.0 mg/dL), and the blood ethyl alcohol concentration level was <0.010%. Toxicology tests using PM blood revealed no significant findings (some drugs, including anti-diabetics, were within therapeutic blood concentration).
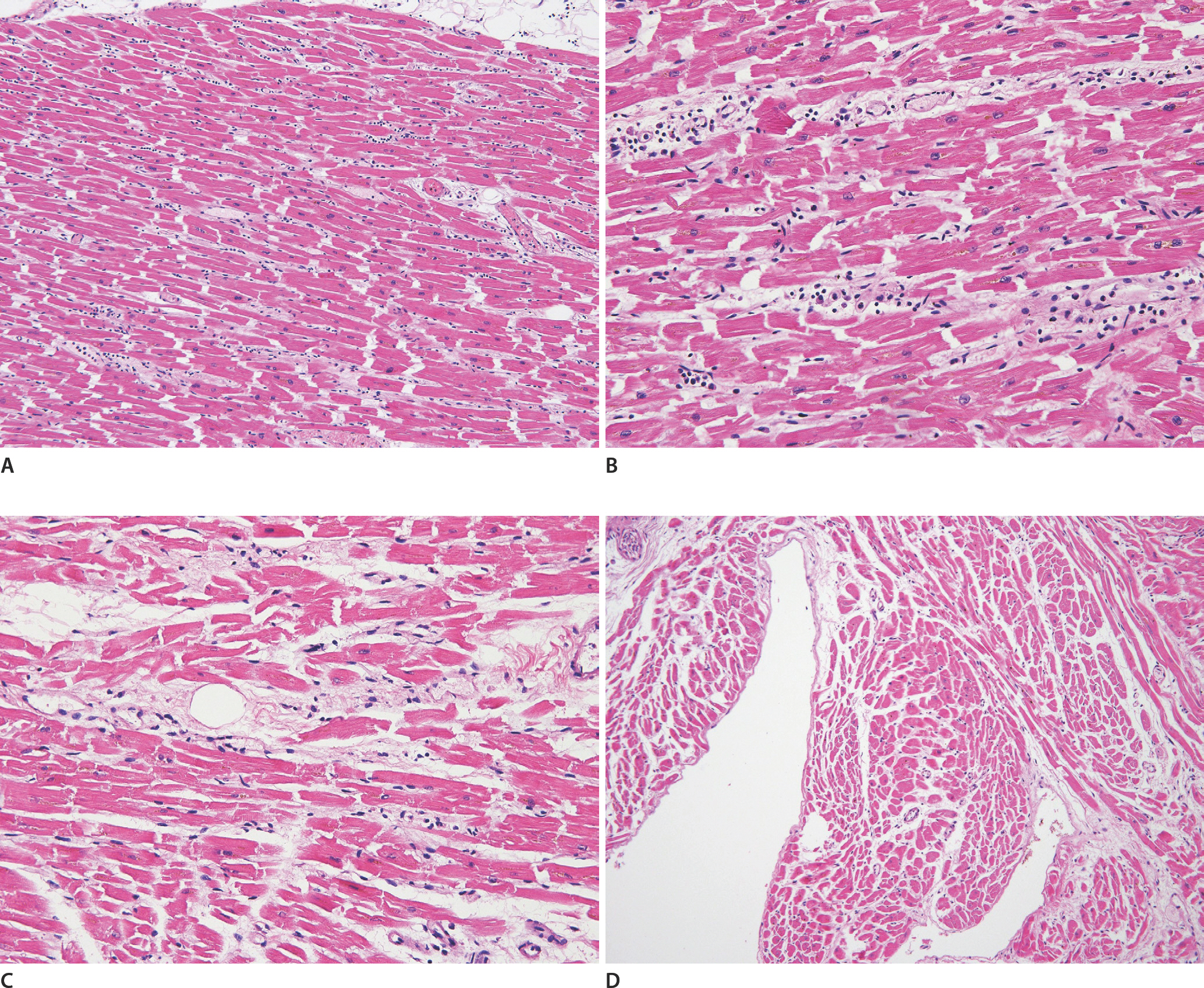
Perivascular lymphocytic infiltration is noted (A, left ventricle, H&E, ×100; B, interventricular septum, H&E, ×200; C, right ventricle, H&E, ×200). No findings of myocarditis were observed in the endocardial and subendocardial tissue (D, H&E, ×100).

Perivascular T-lymphocytic infiltration is noted (A, CD3 with hematoxylin counterstain, ×200). Perivascular CD68+ macrophages are noted (B, CD68 with hematoxylin counterstain, ×200). Heterogeneity of stain is noted, and injured cardiomyocytes demonstrate a relative loss of immunohistochemical staining for desmin. Additionally, counterstained lymphocytes are identified in the adjacent area of injured cardiomyocytes (C, desmin with hematoxylin counterstain, ×200). Injured cardiomyocytes are indicated by purple color, while the surrounding normal cardiomyocytes are indicated by red color for Masson's trichrome stain. Vascular tissue with perivascular lymphocytic infiltration is also identified (D, Masson's trichrome stain, ×100). Black arrows indicate injured cardiomyocytes.

Diffuse alveolar damage with hyaline membranes, intra-alveolar and interstitial edema, and lymphocytic infiltrates are noted in the lung tissue (H&E, ×100).
After comprehensive PM examination, including gross dissection, microscopic examination, PMCT, and PM laboratory tests, the authors concluded that the patient had died of myocarditis caused by COVID-19. Finally, COVID-19 was confirmed as the cause of death, and the manner of death was considered natural.
Discussion
Following the pandemic, the effects of COVID-19 due to the SARS-CoV-2 have been reported with major manifestations being pulmonary complications, including pneumonia [6]. However, the cardiovascular system can also be involved, and cardiac manifestations are critically important because they contribute to a significantly elevated risk of mortality and adversely affect long-term clinical outcomes [1]. Furthermore, cardiovascular involvement can cause SUD, which is commonly observed in forensic medicine. The mechanism of cardiac involvement of SARS-CoV-2 is not fully understood. Cardiac injury may result from various mechanisms, including direct myocardial damage caused by SARS-CoV-2, electrolyte abnormalities, relative ischemia, coronary thrombosis, acute plaque rupture, and cytokine storms [7]. Consequently, cardiac manifestations caused by COVID-19 may be broad and include signs and symptoms of acute heart failure, cardiogenic shock, myocarditis, acute coronary syndrome, a broad range of atrial and ventricular arrhythmias, and cardiac arrest [8]. Among these manifestations, myocarditis is forensically important because it can cause SUD and can be diagnosed based on pathological evaluation. Viral infections such as RNA viruses (Coxsackie viruses A and B, echoviruses, influenza A and B viruses, etc.) and DNA viruses (adenoviruses, cytomegalovirus, Epstein-Bar virus, etc.) are major etiologies of myocarditis, moreover, there are various other etiologies for myocarditis, such as immune-mediated factors (vaccines, heart transplantation rejection, various autoimmune diseases, etc.) and toxins (drugs, heavy metals, radiation, etc.) [5]. The exact pathophysiology of COVID-19–induced myocarditis has not been fully elucidated, and the following mechanisms have been proposed: immune-mediated, autoimmune-mediated, and direct virus-induced myocarditis [4]. In patients with immune-mediated myocarditis, both innate and acquired immune responses contribute to myocardial injury [1]. Autoimmune-mediated myocarditis may develop in response to the release of antigens from cardiomyocytes following a virus-mediated injury [1]. SARS-CoV-2 may invade cardiac myocytes via its surface ACE2 receptors, which may cause direct cellular damage.
No single laboratory test exists to diagnose myocarditis, and pathological tests are useful for diagnosing myocarditis and identifying its etiology. Myocarditis is generally defined as the presence of an inflammatory infiltrate with adjacent cardiomyocyte injury. The infiltrate is lymphocyte-predominant, particularly in cases of viral infection. Occasionally, the dominant cell type in myocarditis is eosinophils or neutrophils. The Dallas criteria for diagnosing myocarditis were developed for endomyocardial biopsy (EMB). However, they have been used for autopsy, and careful histopathologic examination as part of routine autopsy is important for diagnosing myocarditis [9]. In a previous report, unspecified immunohistochemical criteria were proposed for the diagnosis of myocarditis, and abnormal inflammatory infiltrate was defined as ≥14 leukocytes/mm2 including up to 4 monocytes/mm2 in the presence of CD3+ T lymphocytes ≥7 cells/mm2 [5]. The present case met these criteria. In a previous report on COVID-19–induced myocarditis [10], pathological evaluation demonstrated an inflammation of the myocardium with a predominance of macrophages, and cardiomyocyte necrosis was limited. Cases that met the Dallas criteria for myocarditis were infrequent [10]. Perivascular infiltration of lymphocytes and macrophages was identified, which was consistent with the findings of the current study. Moreover, unique myocardial inflammation with or without direct cardiomyocyte damage in COVID-19 myocarditis suggests different pathophysiological mechanisms [10]. Similarly, the presence of cellular infiltrates and necrosis was highly variable, and autopsy findings did not demonstrate a specific, reproducible histopathology of COVID-19 myocardial insult [11]. Therefore, the pathological findings in this case report could present an additional valuable histopathology of COVID-19 myocarditis. Myocarditis sufficient to cause cardiac dysfunction is expected to be diffuse or multifocal with a significant amount of inflammatory infiltration and myocyte injury [11]. In this case lymphocytic infiltration was noted in the left and right ventricles and interventricular septum. Although not diffusely noted, in the present case, injured cardiomyocytes were multifocally identified by immunohistochemical staining for desmin and Masson's trichrome staining [12]. Injured cardiomyocytes were mainly observed in the area adjacent to the perivascular inflammatory infiltration. Although these microscopic findings might not meet the Dallas criteria, they may be sufficient to diagnose myocarditis as the cause of SUD. Nevertheless, we could not exclude that these injured cardiomyocytes caused by other conditions, such as cardiogenic shock. However, the patient complained of syncope after release from isolation, and her CRP levels were elevated in the PM blood sampled during autopsy. We believe that these were pathologic findings related to SUD caused by COVID-19-induced myocarditis.
Previous review articles have rarely reported pathologically identified inflammation in clinically diagnosed cases of COVID-19–induced myocarditis [10,11]. Of the 38 case reports of patients with confirmed COVID-19, EMB was only performed in eight patients [10]. Furthermore, in a previous report of myocarditis after COVID-19 vaccination [13], EMB findings were reported in only two patients who did not demonstrate myocardial lymphocytic infiltration or any evidence of myocarditis. This report suggested that this finding could be attributable to a sampling error or a different injury mechanism from classic direct myocardial infection by the virus [13]. Similarly, no findings of myocarditis in many endocardial and subendocardial areas were noted in this case, indicating that excluding COVID-19 myocarditis using one-focus EMB, which is not repeated, is not appropriate.
Some previous cardiac histopathologic studies on COVID-19 have reported the absence of diffuse lymphocytic myocarditis traditionally observed in viral myocarditis and the presence of CD68+ macrophages in the myocardium [14]. Macrophages are ultrastructurally characterized by cytopathy, membrane damage, and cytoplasmic vacuoles [14]. The hearts of ten patients who died from COVID-19, five of whom had myocarditis, revealed no evidence of lymphocytic myocarditis. They demonstrated a greater number and more diffuse distribution of CD68+ cells than those of matched controls or other hearts with myocarditis, indicating that cells of monocyte/macrophage lineage rather than lymphocytes may be dominant [15]. Furthermore, SARS-CoV-2 viral particles have been detected in interstitial cytopathic macrophages in the myocardium, suggesting that SARS-CoV-2 can reach the heart through infiltration of infected macrophages into the myocardium [14]. Similarly, giant cell myocarditis, which seemingly macrophages play important roles for its pathophysiology, have been reported after vaccination for SARS-CoV-2 [16,17]. These reports suggest that macrophages in the myocardium could play a significant role in developing COVID-19 myocarditis and myocarditis following COVID-19 vaccination. Similar to previous reports, perivascular CD68+ macrophages were observed in the present case. Furthermore, sudden cardiac death caused by small vasculitis after COVID-19 vaccination has been reported [18]. These histopathological similarities suggest similar pathophysiological mechanisms between COVID-19 myocarditis and COVID-19 vaccination induced myocarditis.
As in forensic medicine, proper decisions regarding the cause of death are also important in the field of public healthcare systems. The patient died after being released from isolation, and it would have been plausible that her death was regarded as not related to COVID-19 if proper PM examination, including autopsy, was not performed. However, in the present case, the cause of death was confirmed to be COVID-19 myocarditis after a comprehensive PM examination. This case report highlights the importance of autopsy and proper PM examination in both forensic and public healthcare systems.
Notes
Conflicts of Interest
Joo-Young Na, a contributing editor of the Korean Journal of Legal Medicine, was not involved in the editorial evaluation or decision to publish this article. All remaining authors declare no conflicts of interest.
Acknowledgments
This work was supported by a 2-Year Research Grant of Pusan National University.