낭성 뇌동맥류의 파열과 연관된 전교통동맥의 드문 해부학적 변이
Rare Anatomic Variation of Anterior Communicating Artery Associated with a Rupture of Saccular Aneurysm
Article information

Trans Abstract
Although most cerebral aneurysms are considered as acquired degenerative lesions, diverse anatomical variations in the circle of Willis have been encountered, some of which may play an important role in lesion hemodynamics and pathogenesis. The coalescence of the small vascular plexus to form the anterior communicating artery at the 6-7-week embryological stage may lead to developmental variations, such as fenestration and duplication. Herein, we report a rare anatomical variant of the anterior communicating artery that was concomitantly identified with a ruptured aneurysm. Both the right and left anterior cerebral arteries were connected by three anterior communicating arteries. A vertical segmental artery was present and connected the two anterior communicating arteries, forming an H-shape or plexiform structure. Furthermore, a 0.6×0.4 cm-sized saccular aneurysm with antero-inferior projection was present in the middle anterior communicating artery. The combination of triplication and H-shape in the present case was compared to previously reported anatomical variants.
고 찰
낭성 뇌동맥류의 형성은 후천적 퇴행성 변화에 기인하는 것으로 받아들여지나 윌리스환(circle of Willis)의 다양한 해부학적 변이가 알려져 있으며, 뇌혈관 분지부(bifurcation)에서 보이는 혈관 굵기의 비대칭성은 혈역동학적 부하를 야기하고 뇌동맥류의 형성 및 파열 위험과 관련이 있다고 알려져 있다[1–5]. 저자들은 자발성 지주막하출혈이 사망원인이었던 부검에서 뇌동맥류 파열과 함께 발견된 전교통동맥(anterior communicating artery)의 매우 드문 해부학적 변이에 대해 보고하고자 한다. 변사자는 보통 체격 40세 남자로 오전 10시경 화장실 대변기에 앉은 채 사망한 상태로 발견되었다. 미만성으로 지주막하출혈이 있었고, 전교통동맥에 0.6×0.4 cm의 파열된 뇌동맥류가 있었다(Fig. 1). 양측 전대뇌동맥(anterior cerebral artery) 사이를 수평에 가까운 방향으로 연결하는 전교통동맥이 총 3개가 있었고, 전대뇌동맥과 각 전교통동맥이 만나는 지점은 시신경 교차부(optic chiasm)로부터 전방으로 약 1 cm, 1.2 cm 및 1.7 cm 떨어진 지점에 각각 위치하고 있었다. 동맥류의 경부(neck)는 두 번째 전교통동맥과 우측 전대뇌동맥이 만나는 지점에 있었고, 동맥류의 원개(dome)는 접형골면(planum sphenoideum) 또는 전두부를 바라보는 전하방(antero-inferior projection) 방향성을 보였다. 가장 전방에 위치한 세 번째 전교통동맥은 동맥류 원개에 의해 가려져 혈관을 뇌바닥면으로부터 박리하고 나서야 확인할 수 있었다. 두 번째와 세 번째 전교통동맥은 수직 방향으로 난 혈관에 의해 서로 연결되어서 전체적으로 H 모양을 형성하고 있었다. 휴브너되돌이동맥(recurrent artery of Heubner)은 좌우 전대뇌동맥의 두 번째 전교통동맥과 세 번째 전교통동맥 사이 수준에서 각각 1개가 기시하여 전대뇌동맥A1 분절(precommunicating segment)과 나란한 방향으로 주행하였다. 부검 과정에서 기저 동맥(basilar artery) 부위는 확보되지 않았고, 절제된 윌리스환에서 전교통동맥의 변이 이외에 전대뇌동맥 A1분절의 저형성(hypoplasia)을 비롯한 다른 해부학적 변이는 없었다. 뇌동맥의 가장 좁은 곳의 직경을 측정자로 계측하지는 못했다. 심장은 무게가 440 g으로 경한 심비대가 있고, 관상동맥의 부분적인 중등도 동맥경화증 외에 특별한 병변은 없었다.
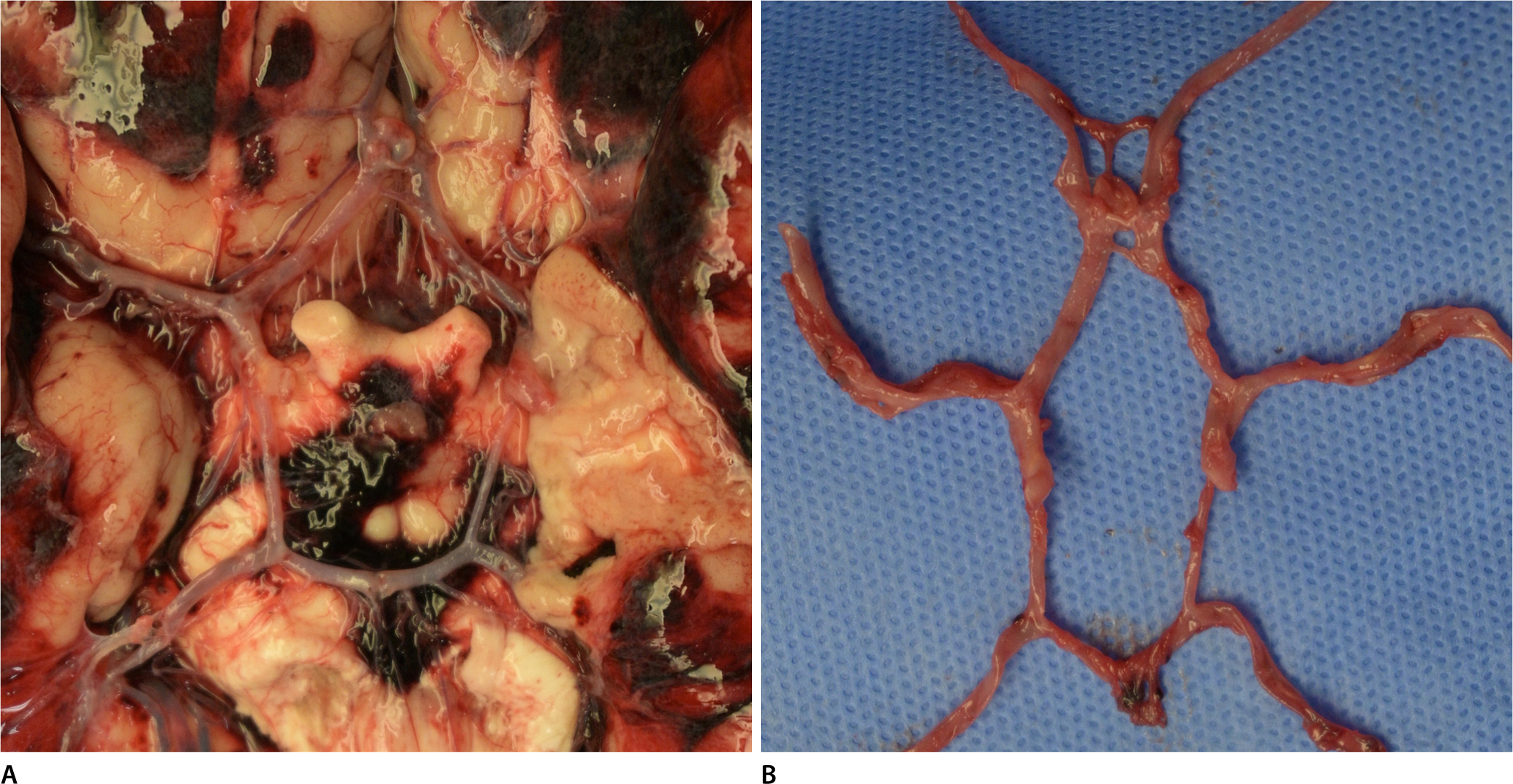
A spontaneous subarachnoid hemorrhage in a 40-year-old man. In the inferior view of the brain, two anterior communicating arteries, along with a ruptured saccular aneurysm, were identified. The aneurysm neck was located in the junction between the right anterior cerebral artery and one of the anterior communicating arteries (A). The dissection of the circle of Willis revealed an additional anterior communicating artery, with a longitudinal segmental channel connecting the two anterior communicating arteries (B).
태생학적으로 윌리스환은 발생 28일 무렵에 원시 내경동맥(primitive internal carotid artery)이 나타나기 시작하고, 발생 6-7주 무렵에 양측 전대뇌동맥으로부터 뻗어져 나온 작은 혈관 얼기(small vascular plexus)들이 서로 합쳐지며 전교통동맥이 만들어지는데, 이러한 과정에서 다양한 해부학적 변이가 전교통동맥에 나타날 수 있다(Fig. 2) [9]. 전교통동맥에 뇌동맥류가 형성되는 경우 다른 곳에 위치한 뇌동맥류에 비하여 파열 위험도가 상대적으로 높다[2]. 전교통동맥의 해부학적 변이에 관한 주요 부검 연구 및 영상의학적 연구들을 정리하면 표1과 같다(Table 1) [3–8]. 연구자별로 변이 유형에 대하여 서로 다른 정의를 사용한 것이 각 변이의 빈도가 다른 원인일 가능성이 있다. Kayembe 등[4]은 Y, V, H 모양과 중복(duplication) 변이, 삼중복(triplication) 변이 및 그물모양(plexiform) 변이를 모두 유창(fenestration) 변이로 지칭하였고, 모식도를 통하여 그물모양 변이는 세 개의 수평방향 전교통동맥에 수직 방향 혈관이 다수 배열되어 있는 형태로 소개하였으나 유창 변이 가운데 그물모양만의 빈도가 어느 정도인지는 제시하지 아니하였다. 반면 De Silva 등[6]은 Y, V, H 모양을 중복의 하위범주로 간주하면서 그물모양 변이는 두 개의 수평방향 전교통동맥 사이에 수직 방향 혈관이 다수 배열된 것을 H 모양과의 차이로 제시하였으나, 그물모양의 구체적 빈도는 제시하지 아니하였다. Kardile 등[7]은 De Silva 그룹과 마찬가지로 그물모양 변이를 두 개의 수평방향 전교통동맥이 기본 구조인 것으로 제시하였고, 그물모양 변이는 3%, 삼중복 변이는 1% 빈도라고 보고하였다. 종합하면, 본 증례처럼 전교통동맥의 수평방향 성분이 3개이면서 두 번째 및 세 번째 수평방향 혈관이 수직방향 혈관으로 이어져 H 모양 또는 그물모양을 이루는 형태는 기존의 보고된 사례와는 차이가 있다. 윌리스환의 변이를 분류하는 통합된 체계가 2021년 제시되었으나 본 증례에 부합하는 정의는 없었다[10]. 영상의학 기술의 획기적인 발전에도 불구하고 부검을 통해 육안적으로 확인하는 해부학적 소견은 여전히 중요하다. 법의부검의 특성상 사망원인 판단과 연관된 소견에 초점이 주로 맞춰지나, 드문 해부학적 변이가 동맥류 파열과 함께 있었던 증례를 소개하고자 한다.

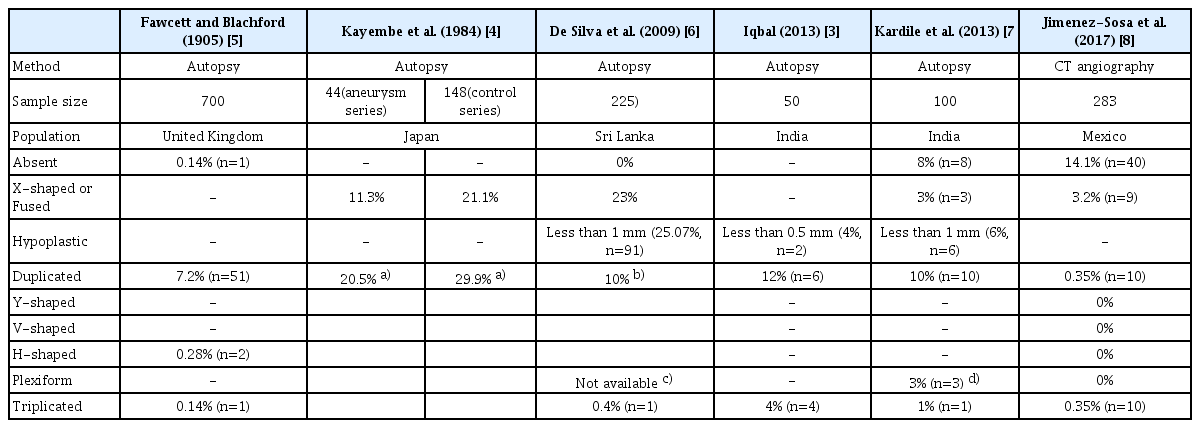
Previously reported anatomic variation of anterior communicating artery
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.